
- In(Fertility) Journey- 1. Introduction
- (In)fertility Journey- 2. Background
- (In)Fertility Journey- 3. Before IVF- Hope
- (In)Fertility Journey- 4. Preparing for IVF
- (In)Fertility Journey- 5. Decisions regarding IVF
- (In)Fertility Journey- 6. IVF Stimulation
- (In)Fertility Journey- 7. IVF Egg Retrieval
- (In)Fertility Journey- 8. IVF After Egg Retrieval
- (In)Fertility Journey- 9. IVF Considerations
After the prep cycle during which I took birth control pills for 22 days, I began the stimulation for IVF. I’ve included my proposed schedule below.

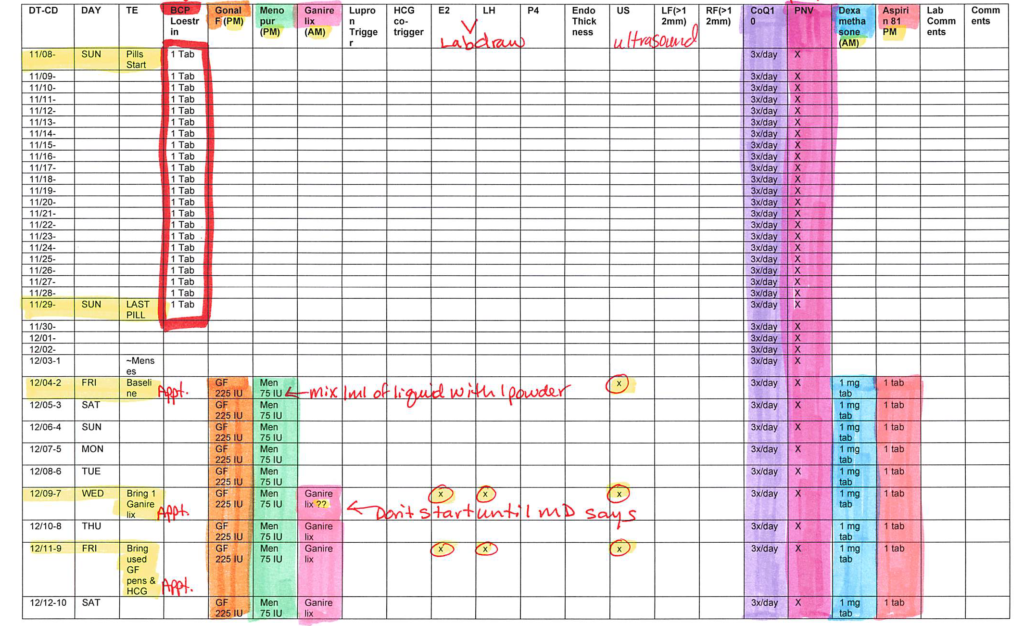
After completing my birth control course, I had an appointment 5 days later to evaluate conditions before starting stimulation. Your period typically begins a few days after the last active birth control pill, and once I started, I had to notify my clinic. However, unlike other cycles, despite the fact that my period started on 12/02, for all further purposes, the Cycle Day number is recorded as assuming my first appointment is ‘Cycle Day 2’ (‘CD2’ in the first column). I suspect this is because the schedule was created during my prep cycle, and they did not want to bother with changing the schedule at the last minute. So while I’ll use the CD designated on my schedule for further discussion, keep in mind that the true CD is actually +1 (my first appointment on 12/04 was actually day 3 of my period, or CD3 despite being designated ‘CD2’ on my chart).
This period after birth control was relatively light. I was so glad to stop the birth control- it just made me all wonky and grumpy.
At my first appointment on ‘CD2’, a female doctor performed a transvaginal ultrasound (tv-US). The observations for both ovaries were that follicles were less than 10mm, there were no cysts, and that it was ‘quiet’. In terms of my uterus, the recorded ‘endo type’ is ‘homogeneous’ and the ‘Cul de Sac Fluid’ was recorded as ‘none’. These were all good signs, so I was approved to begin stimulation. At the end of my tv-US, I met with my nurse coordinator who gave me a demonstration of administrating the Gonal F and Menopur medications via subcutaneous injections in the abdomen area. It really helped that I had already familiarized myself with the process (via the videos available at http://freedommedteach.com/eng/).
I was also directed to take orally 1mg Dexamethasone in the morning, and 81mg of Aspirin in the evening every day.
I was told to try to administer the drugs every evening at the same time, and that this time should be after 6pm. This is to that the clinic would have time to run and analyze any blood tests during the monitoring stage, and adjust the medication dosage the same day if necessary. We set an alarm on our cell phones for 8:30pm, so that we could do the injections around 9pm every evening. This gave us time to eat our dinner, and have my stomach settle a little before I start jabbing myself in the tummy.
Note: I always did my injections while sitting on our living room couch with all the stuff on our cleaned coffee table (we wiped it down with a precious lysol wipe each night before starting). I found this to be helpful because I was really stable and I was less worried about dropping things on the ground and breaking things (I read one woman’s experience of dropping a prefilled syringe and having to buy an additional dose). It was also easy for my husband to keep an eye out for me. It was just easier to examine my tummy to look for an area that I hadn’t poked before and also avoid any veins. Finally, I was pretty careful to be gentle in my injections, but I still got maybe 4 bruises from injections. I wouldn’t pinch myself too hard, I was careful to minimize movement in the 5 seconds after injection before pulling the needle out, and I would do the poke quickly, but not push the needle in further than the approximately 1/2 inch necessary. I felt all this made the injections easier for me.
Gonal-F RFF Redi-ject: 225 IU subcutaneously at the abdomen every evening at 9pm.
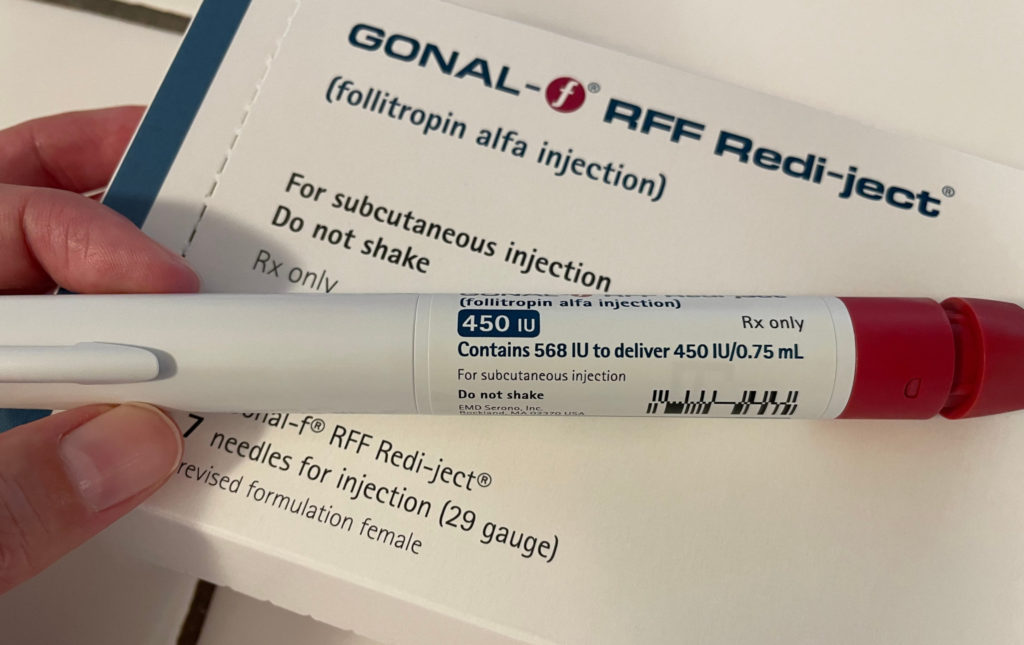
This stuff is expensive! One of the reasons we always began our preparation 30 mins in advance is because this drug is recommended to be taken out of the refrigerator 30 mins before inject to allow to warm to room temperature. So we would prepare this and then do the other injections first while allowing this to reach room temperature. A benefit of this is that at room temperature, the condensation disappears from the syringe, and it’s easier to verify the contents of the syringe.
This medication was relatively easy to administer, check out the video tutorial. I don’t know the gauge of the needle, but it was quite thin, so not too bad. I found it really helpful to have my husband verify that I’ve dialed the correct dose before injecting, and that the dose window shows ‘0’ after. You can also note the position of the plunger and the contents of the syringe before and after administration.
Each Redi-ject pen is loaded with some extra (noted the ‘Contains 568 IU to deliver 450IU/0.75mL’ on the pen). Our clinic told us to refrigerate any used pens, and they were able to collect an additional dose for us, although we actually didn’t end up needing it. But it is so good to know that there is some extra here for wiggle room.
Menopur with Q cap: 75 IU subcutaneously at the abdomen every evening at 9pm.
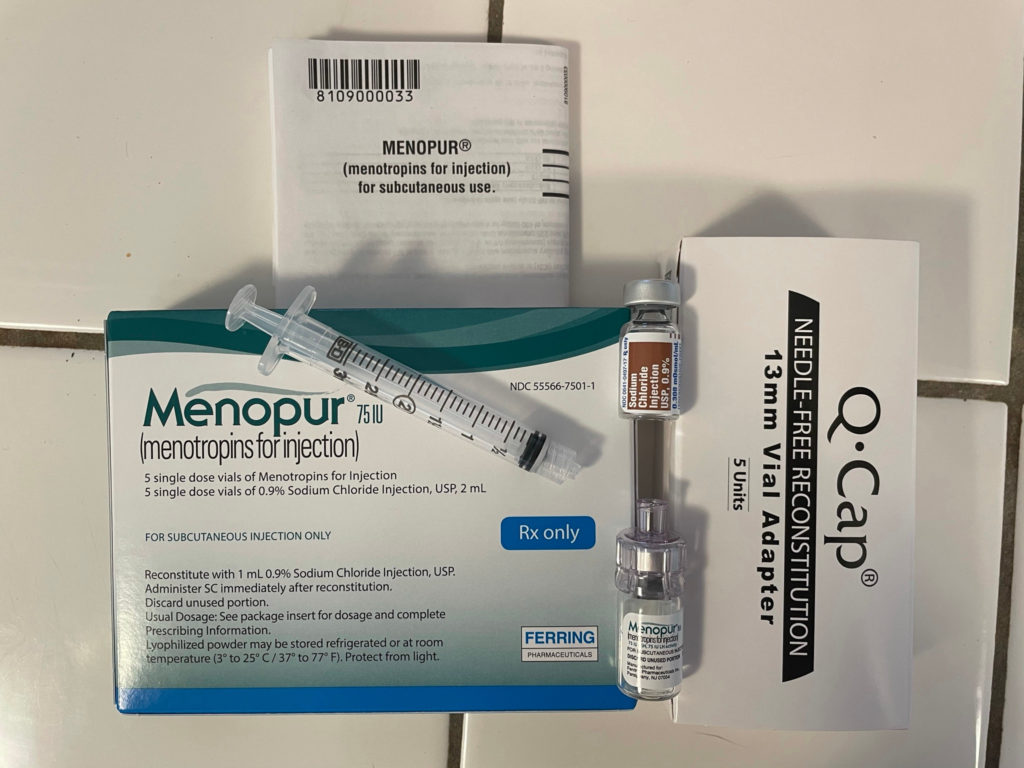
This medication requires a bit of work- You’ll need to reconstitute the medication from the powder and the diluent. Check out the video, here is also a pdf pamphlet. I learned to hold all the parts firmly in the process- the practice with my nurse coordinator was really helpful in getting a feel for how hard to push/pull the Q cap into and out of the rubber gaskets on the bottles.
This is administered with a 27 gauge, 1/2″ needle, which is not bad. However, the medication stings/burns on it’s way in. The area also tends to be a bit tender afterwards. For this reason, I would inject this away from where I injected Gonal-f, just to minimize aggravation- I would inject Gonal-f on the right side of my belly button one night while injecting Menopur on the left side of my belly button, and then switch the next night.
I manage to do all the injections correctly, was just relieved that everything was okay. That night, have a terrible time sleeping. A possible side effect of Dexamethasone is insomnia, not helpful! Got maybe 1-2 hours of sleep that night. Slept about 4 hours in the morning. So glad not to be working during this.
‘CD3’– Felt better about the injections. Slept better than the night before. Feel as though the bloating from the period never really went away.
‘CD4’– Feeling a bit bloated. Usual morning poop not really moving along. Not sure if the inside or the surface of the belly is uncomfortable, but general stomach/abdomen discomfort.
‘CD5’– Inside of the stomach feels a bit better while the surface of the stomach is feeling more tender, am having difficulty remembering where I’ve injected myself before on the abdomen in looking for un-poked regions for injections… Stomach making lots of noises. Unsatisfactory poo, starting to feel more constipated. My husband rubbed my back this evening, so nice! Slept a bit better.
‘CD6’– Feeling general malaise and grumpy. Getting pains in the stomach. Pooped some, so feel a little better, but still not totally caught up. General discomfort is affecting appetite, but I try to eat more hoping the fiber will help with the pooping. Getting random sharp pains in the stomach, don’t know if related to reproductive organs or digestive organs.
At my second appointment on ‘CD7‘ after 5 days of stimulation meds, the same female doctor performed another tv-US, and I had my blood drawn. I was told that the goal is to have the ‘leading’ follicle at a minimum of 14mm. The blood test evaluated both Estradiol and LH, to establish a baseline. The tv-US showed that I had 7 follicles in my left ovary and 6 follicles in my right ovary. The numbers reported are the average of the widest and narrowest distance for each follicle. My endometrial lining was 10.51mm.
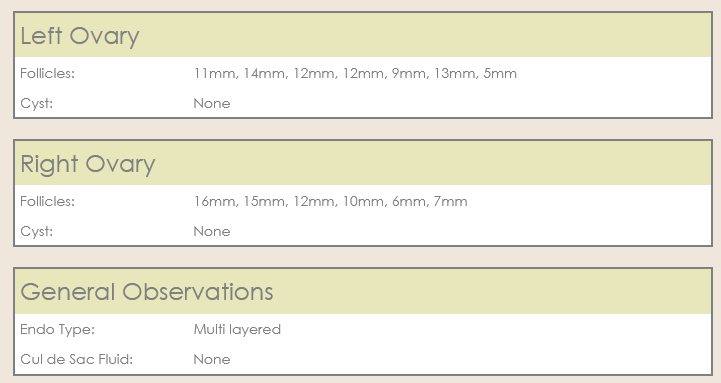


Based on the tv-US, I was told to begin Ganirelix. These results suggests that my IVF cycle was on track. I asked about the Estradiol and LH results, and was told it’s all relative. That they wanted to see my Estradiol go up, and to maintain my LH.
After my tv-US, I met with a different nurse coordinator, who administered my first Ganirelix shot.
Ganirelix Acetate 250 mcg/0.5 ml subcutaneously at the abdomen every morning at 11am.
What’s good about the Ganirelix is that it’s all ready to go in a pre-filled syringe. The bad thing about Ganirelix is that I don’t know what the gauge of the needle is, but it requires a much more deliberate jab to get the needle in. On top of this, Ganirelix also stings/burns after going in, and it continued to hurt for a couple of hours (maybe 4 or so?) afterwards. So depending on whether you’d prefer to space out the painful injects or rather they were on the same side of your abdomen, you can decide whether to always administer the Ganirelix on the same or different side as the Menopur. I didn’t think it was a good idea to mix drugs, and as these two hurt, I assumed my body is reacting, and I didn’t want to amplify the negative reactions so I administered Menopur and Ganirelix on different sides of my abdomen.
Meanwhile, I’m feeling increasingly distended, bloated, and gassy. I find myself sitting down, lying down a lot.
‘CD8’– Still distended and bloated. The pooping situation is a bit worse. I’m having what I call ‘goat poops’, meaning there clumps of little poops, but not a complete evacuation. Getting a bit constipated. Eating lots of fiber and drinking lots of fluids with electrolytes.
At my third appointment on ‘CD9’ after 7 days of stimulation meds, a different male doctor performed another tv-US and I had my blood drawn. This doctor only measured follicles that were ‘large’, he estimated there were about 5 on each side that were of a size that looked likely to retrieve mature eggs.
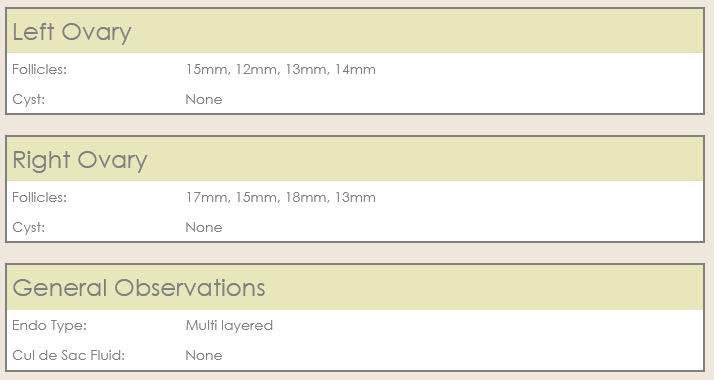


I was told that my lining was ‘over 10mm’, which was good; that a minimum of 7mm is necessary for embryo implantation, so it seems that I won’t be having a problem with growing a uterine lining that can support implantation. I was told that so far I was on track. The goal is that the follicles should grow 1-3mm/day, and my leading follicle from this appointment was 2mm larger than my leading follicle from my previous appointment, which is good, it shows my follicles are still getting bigger. In addition, my Estradiol was going up, which was also a good indicator. My suppressed LH makes sense because that is the job of the Ganirelix, to lower LH to prevent spontaneous ovulation by my body.
Directed to continue the meds. Distended and gassy. My stomach is so uncomfortable, I can’t tell whether it’s my reproductive organs, my intestines (constipation?), or the surface of my abdomen after all the pokes. I start wearing my husband’s sweatpants, pulled up all the way to under my boobs, so that I’m warm and my stomach isn’t getting squeezed. This helped a lot.
‘CD10’– Generally distended and bloated. Still somewhat constipated. Insomnia is worse, which negatively affects my mood. Grumpy. Felt better with salty foods.
I had gotten my flu vaccine (INFS Fluarix quadrivalent) on October 29, 2020, and a few days after that, I had a swelling in my armpit of the same arm. It had slowly gotten less tender over time, but during my stimulation, it got swollen again. I don’t know if it was because I was swelling and retaining water everywhere, or what, but it was disturbing. This tenderness went away after about a week or two.
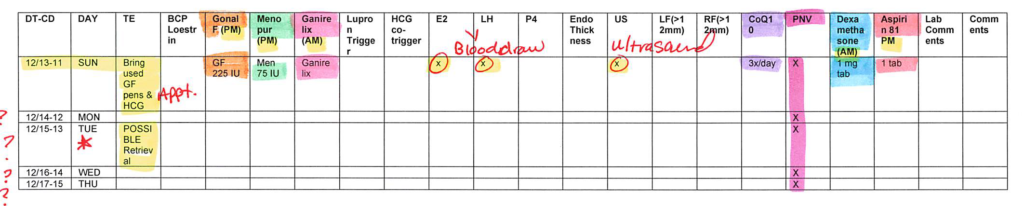
At my third appointment on ‘CD11’ after 9 days of stimulation meds, the same male doctor from the previous appointment perform another tv-US and I get blood work.
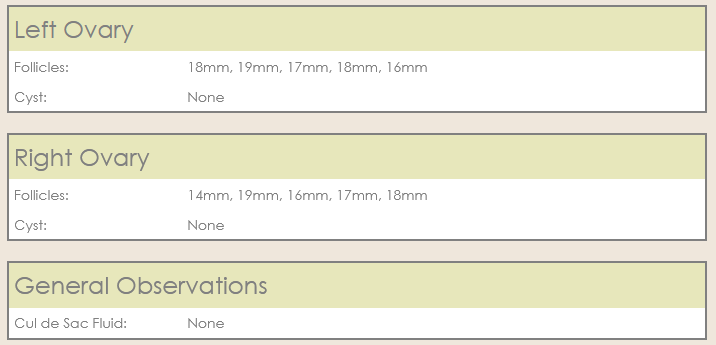


At this point, everything looks on track. The doctor only measured follicles that were ‘large’ and likely to result in a mature egg, so there were more follicles than just the ones measured here. Everything appears on track for egg retrieval on ‘CD13’ as planned. On this day, instead of waiting until evening to take the last injection of Gonal-f, I was directed to take it as soon as we got home after the appointment. So we took the Gonal-f at 11:30am. We continued with Ganirelix, and Dexamethasone, but discontinued Menopur and Aspirin. These are the only changes to the proposed schedule.
That afternoon, the clinic called us with directions to administer the Lupron (Leuprolide) and HCG(Novarel) trigger shot at 11:30pm.
Lupron (Leuprolide acetate) 4mg/80 units subcutaneously at the abdomen in the evening at 11:30pm.
This medication requires you to draw up the correct dosage before administration. Check out the video. This comes with it’s own special syringe so that the correct unit dosage can be administered. I’m not certain, the needle seems to also be 27 gauge and 1/2″ long. Other than drawing out the correct dosage, this injection was pretty straightforward.
I did have a freakout at 11:00pm when I remembered that on of the instructions provided by the clinic that they recommend Lupron to be administered subcutaneously “in the upper outer arm or upper outer thigh”. I was in a panic; this was a super important and timed shot! There was no way I could self administer a shot in the upper outer arm- I wasn’t even sure how to contort myself into position. My husband was clumsy when it comes to fine motor skills even under the best circumstances, and I have skinny arms. I could try to stick myself in the outer thigh, where I did have plenty of subcutaneous fat, but was I even supposed to???!!!
All the demonstrations and instructions I’ve been given thus far had been only for subcutaneous injections in the abdomen. The video instruction on freedommedteach doesn’t even have a video instruction on administration of a subcutaneous injection in the thigh!! After some discussion, my husband and I agreed to go ahead with a subcutaneous injection in the abdomen. The single paper on which the confusing instruction appeared was dated 2008, and it was a good chance that the clinic had not caught that error.
It was fine in the end, but that was a miserable 30mins and for the first time in my life I was drenched with sweat from panic. Up until that point in my life, I had never gotten sweaty in a panic (and I’ve certainly been panicked before!), but during this stimulation, all norms were thrown out the window. Note to self: in the future clarify all injection instructions up front.
HCG (Novarel) 2,500 units subcutaneously at the abdomen in the evening at 11:30pm.
The Novarel I was prescribed comes in a vial freeze dried with 5,000 units, and a vial of diluent. I needed 2,500 units, and I could have reconstituted this myself, but my clinic actually had me bring this to the appointment earlier in the day, and they reconstituted this into a preloaded syringe with 2,500 units. I actually didn’t have to use the syringes/needles, etc., from my drug order. Unfortunately, the needle for the prepared Novarel was not as sharp (?) and like the Ganirelix, I had to jab myself with more *umph*, and I did get a bruise from this poke. Also, my body clearly did not like this, because not only did I get a bruise, but a lump formed at the injection site that did not go away until 2 weeks later.
This evening I was so happy that an end to the injections were in sight. My breasts had begun to get very tender, and I was assured by (a different) nurse coordinator that this was normal, as my estrogen levels are at the highest they’ve ever been.
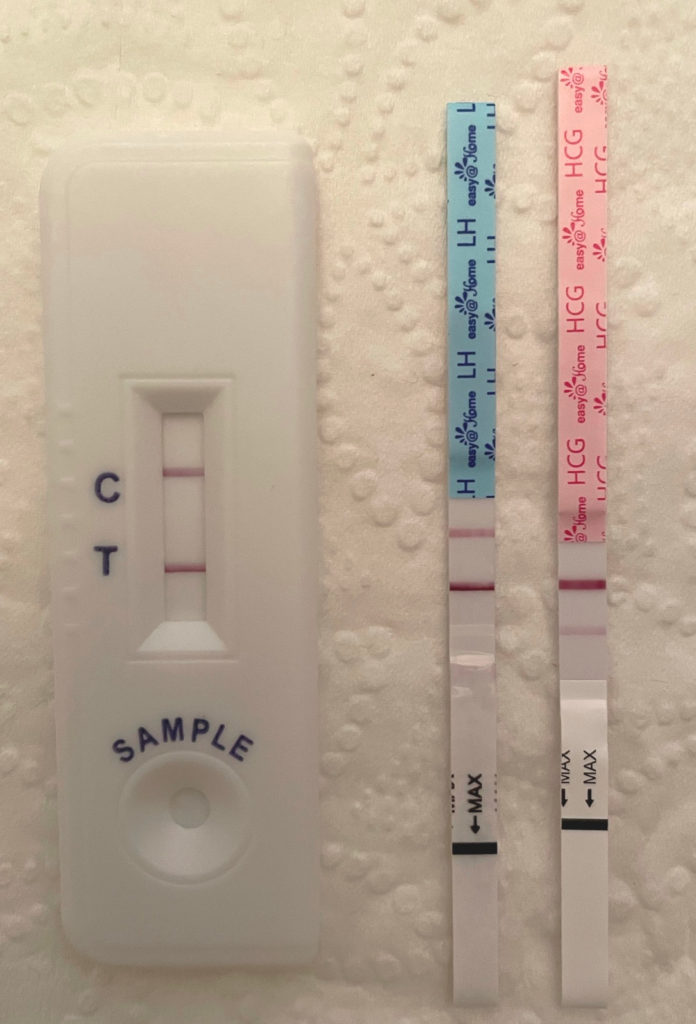
I was also given a urine kit to detect ovulation. I was to test first thing in the morning, and call the clinic if the results were negative by 8:30am latest. If the results were positive, everything was on track.
‘CD12’, I was so relieved to make it to this day! No more medications and only one injection. I was distended and uncomfortable and constipated again. I’ve been having goat poops and rabbit poops (even less than goat poops, little pellets) for the past several days. First thing in the morning I did the urine test, and it was positive, so I was all good.
This evening, I had my last injection: Lupron (Leuprolide acetate) 4mg/80 units subcutaneously at the abdomen in the evening at 11:30pm.
I was expecting to feel a lot worse during this stimulation cycle. I was very uncomfortable throughout it all, but I did not have an incapacitating pain. I was distended, bloated, constipated, achy, tired and grumpy, but manageable.
‘CD13’===> Egg Retrieval, scheduled for 10:30am.
Scaring myself:
Throughout this stimulation protocol I was researching the whole time. In hindsight, I think I did to comfort myself by learning more about the many unknowns in this entire process.
I wondered if and how taking birth control pills that altered my cycle would affect the development of follicles in my ovaries.
I wondered whether there was a significant difference in starting stimulation drugs on CD2 or CD3.
I worried whether taking so much drugs might negatively impact my hormone balance, including my thyroid function, and subsequent ‘fertility’.
I also had totally irrational fears:
Would any of these drugs exacerbate any existing problems in my person?
Would it increase my chances of developing cancer?
Will my hormone-altered body ever return to its former shape and function?
Toward the end of the stimulation cycle, I was sore and bloated but relieved that I wasn’t feeling worse. One of the things we did during the stimulation was nightly weigh-ins for me. A indicator of Overian HyperStimulation Syndrome (OHSS) was weight gain of more than 2lbs per day. My weight fluctuated within 2 pounds during the stimulation, which surprised me, I expected more weight gain. This assured me that I wasn’t heading toward OHSS, and made the discomfort more tolerable.
Another Note: I was warned about constipation, but because I was still pooping a little, I thought I was fine. I was drinking lots of fluids with electrolytes and eating fiber. However, this was not enough, because the constipation got much worse later. More on the next post.
I was a little disappointed that it seems I had only had about 10 follicles that were likely to yield a mature egg, given my AMH and AFC. I was assured that 10 follicles going into an egg retrieval is a perfectly good and reasonable number. So we tried to keep a positive attitude and hope for the best.